There are two threatening clouds for Medicare on the Horizon. One is Ryan and his voucher system. I will get to that shortly. The second is IPAB, the Independent Payment Advisory Board mandated by the new Health Care law.
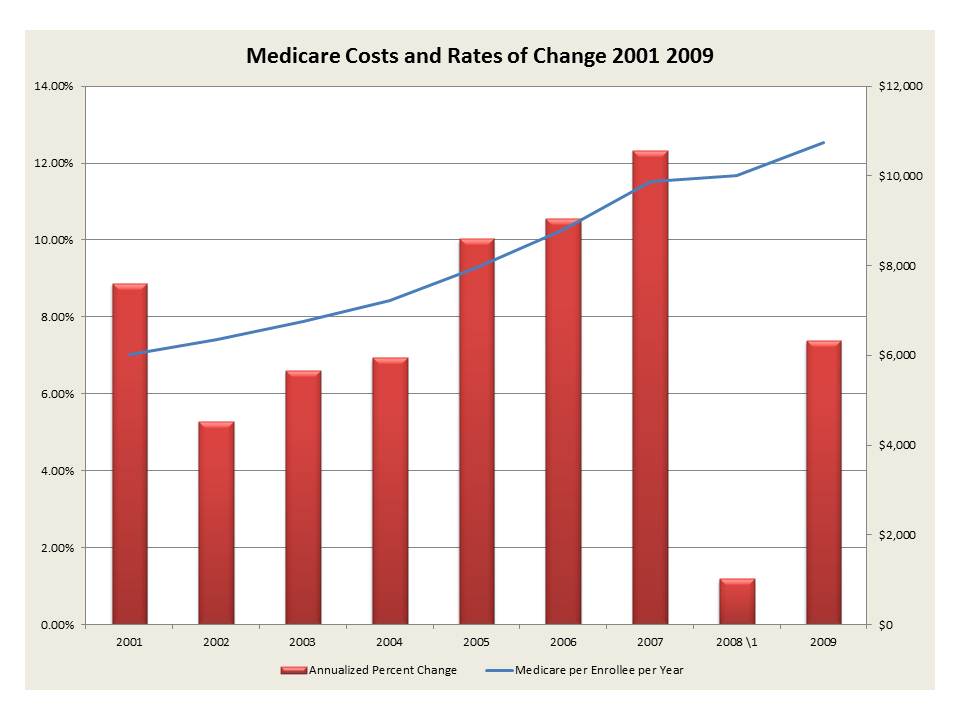
First the Medicare Facts. The chart below based upon Medicare data shows the growth of enrollees and expenditures. Of the almost 48 million enrollees in 2009 about 20% of them are NOT over 65. Frankly they should not be in medicare. They use most of the funds. You see 70% of the Medicare expenditures are used by 10% of the enrollees, and that 20% just mentioned is 90% of that 10%! You see numbers really count.
Now below we show the costs per enrollee per year. That is what Medicare pays, not what it really costs. Beware Government numbers. The annual growth rates are between 6% and 12%, the highest in 2007 for some unexplained reasons from Medicare. But we now spend $10,500 per annum per recipient. Remember that and remember the growth rate, Ryan does not seem to remember that, because he places that on the backs of those who already paid in!
Now let us look at a simple example.
1. Let us take our simple example of a real worker, say a high school teacher, a police officer, not one of the highly paid Boston ones, but say a New York patrolman. They start work in say 1970 and retire in 2010. They start at say $12,000 pa after their Rookie Year and then work a real 40 years till 65. They get paid say $105,000 in their final year. Not unreasonable, unless of course you are in Boston and have packed your final year with excess overtime watching man holes.
2. Now assume you paid 3% of your pay each year to some fund, any fund other than the Government, and the fund invested in say Treasury bonds, notes, Ginnie Maes, whatever. The average return would be well in excess of 5% pa. So by 2010 you have $170,000 in that account.
3. Now you retire. You statistically have 12 years left to live. Yes, that is all, some will live longer some less, but you can bet that the average in this large group is 12.
4. Let us assume that health care can be capped at say 6% annual increase and that it starts at $12,000 pa. You can make book on the fact that on average it will cost $127,000 present value to pay for these expenses. Yes, that is $43,000 LESS than what you contributed. But it gets worse you see, since you are also paying $1,200 pa in addition, which is a present value at 65 of say $20,000. That means you are stiffed for not $43,000 but $63,000! Paul Ryan where are you!
5. Now along comes
Ryan who proposes:
"When fully phased in, the average payment is $11,000 per year (the average amount Medicare currently spends per beneficiary), and is indexed for inflation by a blended rate of the CPI and the medical care component of the CPI. For affected beneficiaries, the payment replaces all components of the current Medicare Program (Medicare fee-for-service, Medicare Part B, Medicare Advantage, and Medicare Part D). Payment amounts are income-related and risk-adjusted. They also are partially geographically adjusted, with the geographic adjustment phasing out over time."
Why do we not get what we put in! The Ryan Plan clearly sets an instant gap! Medical costs are increasing and the increase if due highly to the people in Medicare who should not be. Do we kick them out? What of all that money we put in? Many left wing haters of the old argue that Medicare beneficiaries are getting a free ride, even some ersatz right wing folks, because some number cruncher took the lower decile of workers and showed they get a free ride. Yes, if you worked at McDonald's as a floor sweep for your entire career you would benefit. But if you did you most likely have other problems as well and may not make it 12 years!
Now the current Health care Plan has a number of equally troubling issues the most troubling for Medicare is the IPAB. As stated in
NEJM:
The ACA alters the landscape for control of federal health care spending by creating new institutions
intended to facilitate progress toward reform and by directly altering payment formulas for Medicare and Medicaid. The new Independent Payment Advisory Board (IPAB) and the Center for Medicare and Medicaid Innovation are charged, respectively, with stewardship of Medicare spending and piloting and diffusion of payment and delivery-system reforms. The IPAB is required to recommend
cost-saving measures for Medicare in years when spending growth exceeds a set target; the changes must be adopted unless equivalent alternatives are substituted or Congress intervenes.
As the CBO stated in December 2009:
The legislation would establish an Independent Payment Advisory Board, which would be required, under certain circumstances, to recommend changes to the Medicare program to limit the rate of growth in that program’s spending. Those recommendations would go into effect automatically unless blocked by subsequent legislative action. In its original estimate, CBO wrote that: “Such recommendations would be required if the Chief Actuary for the Medicare program projected that the program’s spending per beneficiary would grow more rapidly than a measure of inflation (the average of the growth rates of the consumer price index for medical services and the overall index for all urban consumers).” That statement is correct for fiscal years 2015 through 2019. After 2019, however, the threshold for Medicare spending growth that would trigger recommendations for spending reductions would be higher—specifically, the rate of increase in gross domestic product (GDP) per capita plus 1 percentage point.
With this corrected reading, savings from changes to the Medicare program (along with other changes to direct spending that are not associated directly with expanded insurance coverage) would increase at a rate that is between 10 percent and 15 percent per year during the 2020–2029 period, compared with a growth rate of nearly 15 percent reported in the initial estimate. The long-run budgetary effects of the other broad categories of the legislation are unchanged from the initial estimate. All told, CBO expects that the legislation, if enacted, would reduce federal budget deficits over the decade after 2019 relative to those projected under current law—with a total effect during that decade that is in a broad range between one-quarter percent and one-half percent of GDP. In comparison, the extrapolations in the initial estimate implied a reduction in deficits in the 2020–2029 period that would be in a broad range around one-half percent of GDP. The imprecision of these calculations reflects the even greater degree of uncertainty that attends to them, compared with CBO’s 10-year budget estimates. The expected reduction in deficits would represent a small share of the total deficits that would be likely to arise in that decade under current policies.
In effect the IPAB becomes a de facto rationer of health care for those on Medicare. They are NOT medical practitioners, they are politicians! Have we not learned anything over the past couple of years? Do we really want to leave choices for life saving procedures to those who could not find employment elsewhere?