Autophagy is the process whereby a cell cleans up the
"stuff" left behind by many processes. However autophagy is also involved
in many cancers and can be a target for a variety of therapeutics. Moreover
autophagy sends out parcels of cleaned up "stuff" which can
themselves be either diagnostic or prognostic. We examine some of these issues
herein.
However, autophagy can be a benefit and a threat. Autophagy
"cleans" up the "stuff" in a cell so that in most cases it
can be recycled and reused. However the risk is that if the autophagy takes up
key protective proteins thus reducing their efficacy and pays no attention to
bad proteins which are now controlling the cell. That is we know that cancer
cells have aberrant proteins. We all too often ascribe this to some genetic
breakdown. What if, instead, it is the clean-up mechanism of autophagy. Namely
every time a p53 gene creates a protein that the specific autophagy targets it
for removal. Then we have a cell with no control.
Thus the questions we should be asking regarding autophagy
are:
1. What are the dynamics of the process?
2. What makes a protein a target? How does the autophagy
process recognize it and why?
3. How do some proteins manage to avoid autophagy?
4. How could we envision a method to control or remedy a
process?
We can envision the autophagy process as shown simply below.
It functions of collecting and degrading old proteins, as an example, returning
them to nucleic acids, to be used again. It is an internal process of a cell to
maintain homeostasis. However like all cell processes it may go awry, and no
longer function efficaciously but be harmful.

Unlike most papers in the field we do not intend to
introduce new ideas or findings but we attempt to concentrate on the above
questions.
From a sequential perspective autophagy as per Kang et al
progresses as follows:

The initiators are as shown below:
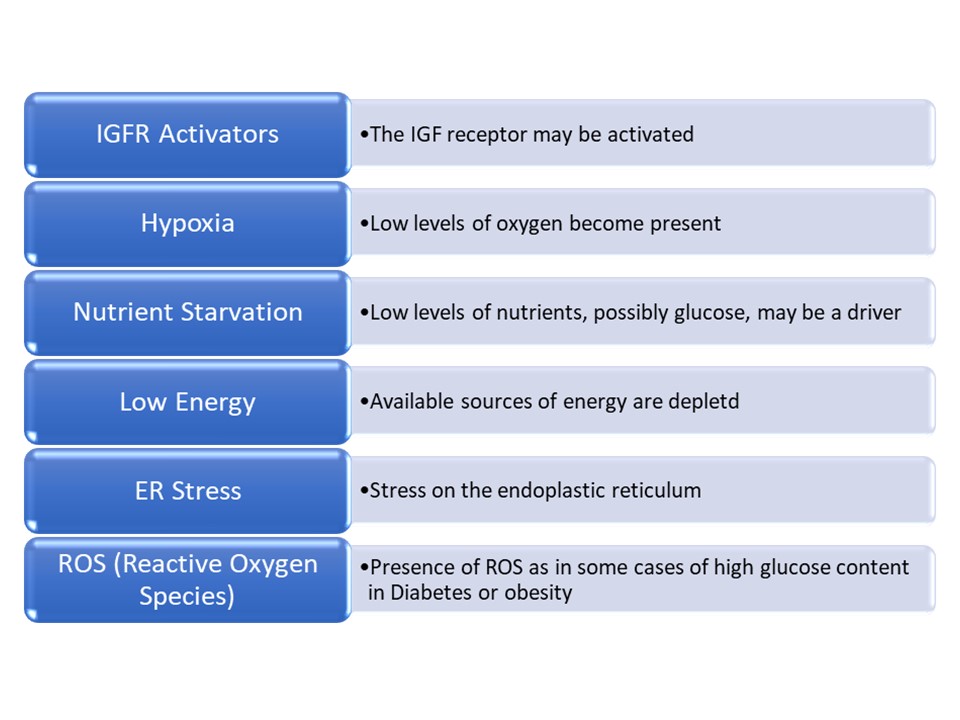
As Kang et al note:
There are at least three different types of autophagy
described and possibly more. These autophagy types include macro autophagy
(hereafter referred to as autophagy), micro autophagy and chaperone mediated autophagy.
The initial step of autophagy is the surrounding and sequestering of
cytoplasmic organelles and proteins within an isolation membrane (phagophore).
Potential sources for the membrane to generate the phagophore include the Golgi
complex, endosomes, the endoplasmic reticulum (ER), mitochondria and the plasma
membrane.
The nascent membranes are fused at their edges to form double-membrane
vesicles, called autophagosomes. Autophagosomes undergo a stepwise maturation
process, including fusion with acidified endosomal and/or lysosomal vesicles, eventually
leading to the delivery of cytoplasmic contents to lysosomal components, where
they fuse, then degrade and are recycled.
One of the issues that we seem to be lacking insight on, is
in the case of autophagy in cancer, either as cause or result, what process
leads to the selection of what is to be lysed. We have great insight to the
process but little to none as to the initial selection. That will be a critical
factor.
From a recent paper by Mulcahy et al we have[2]:
Autophagy is a mechanism by which cellular material is
delivered to lysosomes for degradation, leading to the basal turnover of cell
components and providing energy and macromolecular precursors. Autophagy has
opposing, context-dependent roles in cancer, and interventions to both
stimulate and inhibit autophagy have been proposed as cancer therapies. This
has led to the therapeutic targeting of autophagy in cancer to be sometimes
viewed as controversial. … we suggest a way forwards for the effective
targeting of autophagy by understanding the context-dependent roles of
autophagy and by capitalizing on modern approaches to clinical trial design.
We shall not focus in detail on their suggestions but try to
examine autophagy in general so as to better understand the process.
Yoshinori Ohsumi received the Nobel Prize in Physiology or
Medicine in 2016 for his work on autophagy. He spent decades trying to
understand the process and its implications. In his presentation he noted[3]:
Life is in an equilibrium state between synthesis and
degradation of proteins: replacement of most proteins every 3 months
“difference between organisms and machine”
Recycling is essential for life: important ability for
survival against starvation critical selection factor in evolution.
To Ohsumi the process of autophagy was one of regeneration
not just simple housekeeping. However we know that cells operate as a complex
set of internal mechanisms as well as responding to external activations.
Furthermore cells send out in exosomes "messages" which in turn may
control the behavior of other cells. Autophagy is a process that appears to be
very much in the middle of these communications links. It is a transformative
process, transforming putative signalling molecules to other putative
signalling molecules.
Autophagy appears not to be a simple cleaning up system but
a complex element in an ever more complex control system for cellular dynamics.
Viewed in this manner we extend what Ohsumi understood to the broader
understanding of malignancy control.
As Sengupta et al note in examining mTOR:
Autophagy is a recycling process through which cells
liberate intracellular stores of nutrients by degrading cytoplasmic proteins
and organelles in lysosomes. In mammalian cells the primary form of autophagy
is macroautophagy (referred to from now on as autophagy) and requires the
formation of double-membrane autophagosomes that sequester cytoplasmic
components and then fuse with lysosomes. A major regulator of autophagy is
mTORC1, which in the presence of nutrients and growth factors strongly inhibits
the initiation of autophagy.
Autophagy is upregulated during periods of starvation or
growth factor withdrawal, as well as in response to oxidative stress,
infection, or the accumulation of protein aggregates. While mTORC1 inhibition
triggers autophagy, the release of amino acids from autophagic protein
degradation eventually leads to the reactivation of mTORC1, which in turn
restores the cellular lysosomal population.
Directly downstream of mTORC1 are numerous proteins that
are required for the execution of the autophagic program, including the
serine/threonine kinase Atg1/ULK, which plays a key role in the formation of
the preautophagosome . ULK1 forms a complex with Atg13 and FIP200, which
promote ULK1 kinase activity and localization to the preautophagosome.
mTORC1 phosphorylates ULK1 and Atg13, moderately reducing
ULK1 kinase activity but not affecting its association with Atg13 and FIP200.
Reports conflict about whether mTORC1 binds to the complex under
nutrient-replete conditions, and more evidence is needed to determine the role
mTORC1 phosphorylation of ULK1 plays in its subcellular localization and
interaction with other autophagy proteins. As a result, it is too early to know
whether these phosphorylation events fully explain the control of autophagy by
mTORC1. Interfering with the ability of cells to undergo autophagy within an
intact animal produces a range of phenotypes that underscore the importance of
autophagy not only as an adaptive response to nutrient stress, but also in
general cell and tissue housekeeping.
For example, mice lacking Atg5, which is required for
autophagosome formation, are born at mendelian ratios, but die within 1 day of
delivery because they are unable to mobilize the energy and nutrient stores
they require to survive the pre-suckling period. Mice depleted of Atg5 in just
neural cells exhibit a progressive decline in motor activity that correlates
with the buildup of protein aggregates in neurons, indicating that autophagy is
essential for the basal clearance of these aggregates and to maintain proper
neuronal function in adult animals.
Tissue-specific deletions of additional genes required
for autophagy have uncovered roles for autophagy in cardiac contractility,
immune cell function, and the liver detoxification of drugs.
We can now make some observations regarding autophagy and
cancer.
1. Autophagy as a process is somewhat well understood once it
commences and following through completion. However autophagy as a means to
inhibit or promote cancers does not seem to be well understood at the
initiation stage.
We have examined several putative autophagic related cancer
treatments which we will comment on latter. However most of these are on off
approaches and a general systematic approach does not seem forthcoming.
2. Autophagy as a therapeutic target may have potential for
silencing gene products which facilitate the expansion of certain malignancies.
For example Baquero et al note:
In chronic myeloid leukemia (CML), tyrosine kinase
inhibitor (TKI) treatment induces autophagy that promotes survival and
TKI-resistance in leukemic stem cells (LSCs).
In clinical studies hydroxychloroquine (HCQ), the only
clinically approved autophagy inhibitor, does not consistently inhibit
autophagy in cancer patients, so more potent autophagy inhibitors are needed.
We generated a murine model of CML in which autophagic flux can be measured in
bone marrow-located LSCs.
In parallel, we use cell division tracing, phenotyping of
primary CML cells, and a robust xenotransplantation model of human CML, to
investigate the effect of Lys05, a highly potent lysosomotropic agent, and
PIK-III, a selective inhibitor of VPS34, on the survival and function of LSCs.
We demonstrate that long-term haematopoietic stem cells (LT-HSCs:
Lin−Sca-1+c-kit +CD48−CD150+) isolated from leukemic mice have higher basal
autophagy levels compared with non-leukemic LT-HSCs and more mature leukemic
cells.
Additionally, we present that while HCQ is ineffective,
Lys05-mediated autophagy inhibition reduces LSCs quiescence and drives myeloid
cell expansion. Furthermore, Lys05 and PIK-III reduced the number of primary
CML LSCs and target xenografted LSCs when used in combination with TKI
treatment, providing a strong rationale for clinical use of second
generation autophagy inhibitors as a novel treatment for CML patients with LSC
persistence.
Cristofani et al note regarding prostate cancer:
Within tumour mass, autophagy may promote cell
survival by enhancing cancer cells tolerability to different cell stresses,
like hypoxia, starvation or those triggered by chemotherapic agents.
Because of its connection with the apoptotic pathways, autophagy has been
differentially implicated, either as prodeath or prosurvival factor, in the
appearance of more aggressive tumours. Here, in three PC cells (LNCaP, PC3,
and DU145), we tested how different autophagy inducers modulate
docetaxel-induced apoptosis. We selected the mTOR-independent disaccharide
trehalose and the mTOR-dependent macrolide lactone rapamycin autophagy
inducers. In castration-resistant PC (CRPC) PC3 cells, trehalose specifically
prevented intrinsic apoptosis in docetaxel-treated cells. Trehalose reduced the
release of cytochrome c triggered by docetaxel and the formation of aberrant
mitochondria, possibly by enhancing the turnover of damaged mitochondria via
autophagy (mitophagy). In fact, trehalose increased LC3 and p62 expression,
LC3-II and p62 (p62 bodies) accumulation and the induction of LC3 puncta. In
docetaxel-treated cells, trehalose, but not rapamycin, determined a perinuclear
mitochondrial aggregation (mito-aggresomes), and mitochondria specifically
colocalized with LC3 and p62-positive autophagosomes.
In PC3 cells, rapamycin retained its ability to activate
autophagy without evidences of mitophagy even in presence of docetaxel.
Interestingly, these results were replicated in LNCaP cells, whereas trehalose
and rapamycin did not modify the response to docetaxel in the ATG5-deficient
(autophagy resistant) DU145 cells. Therefore, autophagy is involved to alter
the response to chemotherapy in combination therapies and the response may be
influenced by the different autophagic pathways utilized and by the type of
cancer cells.
3. Autophagy products may allow for liquid biopsy targets for the
purpose of ascertaining diagnostic or prognostic targets.
We have discussed liquid biopsy approaches.
4. Can the gene and gene products in autophagy be used as targets to
mitigate certain types of cancers?
Some effort has been tried on this area and a great deal
more is required.
5. Is there some approach that can be facilitated via immunotherapy?
6. Are there viral vectors which can be employed to facilitate autophagic
controls?
7. What is the impact of obesity and autophagy on cancer presentation?
Obesity has been and is a major source of morbidity and
mortality. It has further become a topic with some significant social backlash
for a physician. Whereas smoking could be called out and managed obesity has
become a personal statement protected by those who often have no understanding
of its risks.
Noa Zhang et al note:
Obesity poses a severe threat to human health, including
the increased prevalence of hypertension, insulin resistance, diabetes
mellitus, cancer, inflammation, sleep apnoea and other chronic diseases.
Current therapies focus mainly on suppressing caloric intake, but the efficacy
of this approach remains poor. A better understanding of the pathophysiology of
obesity will be essential for the management of obesity and its complications.
Knowledge gained over the past three decades regarding the aetiological
mechanisms underpinning obesity has provided a framework that emphasizes energy
imbalance and neurohormonal dysregulation, which are tightly regulated by
autophagy. Accordingly, there is an emerging interest in the role of autophagy,
a conserved homeostatic process for cellular quality control through the
disposal and recycling of cellular components, in the maintenance of cellular
homeostasis and organ function by selectively ridding cells of potentially
toxic proteins, lipids and organelles.
Indeed, defects in autophagy homeostasis
are implicated in metabolic disorders, including obesity, insulin resistance,
diabetes mellitus and atherosclerosis. In this Review, the alterations in
autophagy that occur in response to nutrient stress, and how these changes
alter the course of obesogenesis and obesity-related complications, are
discussed. The potential of pharmacological modulation of autophagy for the
management of obesity is also addressed.
1) Abraham et al, Autophagy as a Possible Target for Cancer Therapy,
J Orthop Oncol 2018, 4:2
2) Baquero, et al, Targeting quiescent leukemic stem cells using
second generation autophagy inhibitors, Leukemia, Nature, https://doi.org/10.1038/s41375-018-0252-4
3) Cristofani et al, Dual role of autophagy on docetaxelsensitivity
in prostate cancer cells, Cell Death and Disease (2018) 9:889
4) Dang and Kim, Convergence of Cancer Metabolism and Immunity: an
Overview, Biomol Ther 26(1), 4-9 (2018)
5) Denny et al, Exploring autophagy with Gene Ontology, Autophagy,
2018, Vol. 14, No. 3, 419–436
6) Hu et al, Targeting Autophagy for Oncolytic Immunotherapy, Biomedicines
2017, 5, 5;
7) Hayat, Autophagy, Academic Press (San Diego) 2014
8) Kang et al, The Beclin 1 network regulates autophagy and
apoptosis, Cell Death and Differentiation (2011) 18, 571–580
9) Kwan and Wai, Autophagy in Multidrug-Resistant Cancers, http://dx.doi.org/10.5772/64274,
Intech, Autophagy in Current Trends in Cellular Physiology and Pathology, 2016
10) Marinkovic et al, Autophagy Modulation in Cancer: Current
Knowledge on Action and Therapy, Oxidative Medicine and Cellular Longevity,
Volume 2018, Article ID 8023821, 18 pages
11) Marx, Autophagy: Is It Cancer’s Friend or Foe?, Science Vol 312
26 May 2016 pp1160-1161.
12) Meiling-Wesse, The Identification and Characterization of six
novel ATG genes, Thesis, Institut für Biochemie der Universität Stuttgart, 2009
13) Mulcahy et al, Targeting autophagy in cancer, Nature Reviews
Cancer Y7, 528-542 (2017)
14) Namkoong et al, Autophagy Dysregulation and Obesity-Associated
Pathologies, Mol. Cells 2018; 41(1): 3-10
15) Ohsumi, Y, Autophagy, Nobel Lecture 2016.
16) Paquette, et al, mTOR Pathways in Cancer and Autophagy, Cancers
2018, 10, 18
17) Rabinowitz and White, Autophagy and Metabolism, Science, Vol 330
3 Dec 2010
18) Rao, Autophagy: a programmed cell death, Arch Gen Int Med, 2017,
V1 No 1
19) Sengupta et al, Regulation of the mTOR Complex 1 Pathway by
Nutrients, Growth Factors, and Stress, Molecular Cell 40, October 22, 2010
20) Yu et al, Autophagy: novel applications of nonsteroidal
anti-inflammatory drugs for primary cancer, Cancer Medicine 2018; 7(2):471–484
21) Zhang et al, Targeting autophagy in obesity: from
pathophysiology to management, Nature Reviews Endocrinology Volume 14, pages 356–376
(2018)
[1]
See https://www.cancer.gov/publications/dictionaries/cancer-terms/def/igfr A protein found on the surface of some
types of cells that binds to insulin-like growth factor (IGF). This causes the
cells to grow and divide. IGFR is found at high levels on the surface of
several types of cancer cells, which causes these cells to grow rapidly in the
presence of IGF. Also called insulin-like growth factor receptor.
[2] Targeting
autophagy in cancer, Jean M. Mulcahy Levy, Christina G. Towers & Andrew
Thorburn Affiliations I Corresponding author, Nature Reviews Cancer Y7, 528-542
(2017) I doi:10.1038/nrc.2017.53, Published online 28 July 2017


